(Resident comes from other rotation, speaks to fellow)
Resident: Teach me something.
Fellow: (sums up case) So CD30 is all you need.
Me: I thought love was all you need.
Resident: Is she always like this?
Fellow: Yes.
Apr 30, 2012
Apr 23, 2012
The Economy Car Blues
I finally got my wonderful guitar gift fixed up for the low low price of 10 dollars, so I can put this to music:
9 AM, the flames are lickin'
10 AM, the porch ain't there
At noon, I'm getting that call saying, girl you're gonna stay where?
And you got no way to get going now,
Naw, they burned up your ride too,
Now I'm sitting in the ruins singing the economy car blues, baby...
Can't get to work
Can't get to church
I'm in the lurch
Can't head to the Red Cross
Can't get to tell my boss
Can't get to the downtown, feeling lowdown blues...
No, I've got the economy car blues.
Where's your bed baby?
That futon? It's gone
Your tv and vodka bottles?
Just pieces on the lawn
But I'm sleeping out here barefoot; yeah they got my pretty shoes,
And now all I got are these economy car blues, yeah
Those subcompact blues,
Those window-crank blues.
When you're missing your stride, you got no ride
Want your stereo, want those sexy pleather seats back
A three quarter spare, smells like burning hair,
and the paint job's turned smoky black
That's just the economy car blues, yeah it is
That's just the economy car blues.
Can't get to work
Can't get to church
I'm in the lurch
Can't get to the mall, not the justice hall
Not the clinic, I can't win it blues
I got these economy car blues. Yeah yeahhhhhhh CHA.
(guitar slide)
---
See, this is what happens when I don't get enough sleep and get called out in derm lecture.
9 AM, the flames are lickin'
10 AM, the porch ain't there
At noon, I'm getting that call saying, girl you're gonna stay where?
And you got no way to get going now,
Naw, they burned up your ride too,
Now I'm sitting in the ruins singing the economy car blues, baby...
Can't get to work
Can't get to church
I'm in the lurch
Can't head to the Red Cross
Can't get to tell my boss
Can't get to the downtown, feeling lowdown blues...
No, I've got the economy car blues.
Where's your bed baby?
That futon? It's gone
Your tv and vodka bottles?
Just pieces on the lawn
But I'm sleeping out here barefoot; yeah they got my pretty shoes,
And now all I got are these economy car blues, yeah
Those subcompact blues,
Those window-crank blues.
When you're missing your stride, you got no ride
Want your stereo, want those sexy pleather seats back
A three quarter spare, smells like burning hair,
and the paint job's turned smoky black
That's just the economy car blues, yeah it is
That's just the economy car blues.
Can't get to work
Can't get to church
I'm in the lurch
Can't get to the mall, not the justice hall
Not the clinic, I can't win it blues
I got these economy car blues. Yeah yeahhhhhhh CHA.
(guitar slide)
---
See, this is what happens when I don't get enough sleep and get called out in derm lecture.
Apr 17, 2012
Meanwhile, in hemelandia
I don't even watch Portlandia much, but I really like adding "ia" onto everything. And putting a bird on it (Okay, I watch Portlandia a little).
Anyhoo: Dear Clinicians, we do actually read your notes. And you are hilarious. "The patient is obese, and extra personnel will be needed in the OR to deal with the obesity of the patient, who I may have mentioned, is obese."
Also, all notes begin "The patient is a pleasant blah blah blah. And all the referrals begin with "Thank you Dr. ScaryName for referring your patient, who is a pleasant blah blah blah". Sometimes, they're "very pleasant". Which of course, is meaningless to us, and after reading thirty notes that begin that way, is either a complete lie, or we have the most pleasant group of in-pain people ever. "The patient, Ms. Jones, is a demanding chore of a woman who has threatened to sue me five times. By referring her to me, I can only guess I have grievously wronged you in some way, and for that, I do apologize."
I know as a medical student, I got some unpleasants. One wanted to be her doctor, which is a story for later and helped me run screaming into my field just in case she ever found me. "My patient, Ms. Really?, said she threatened to slap a nun. I feel no further history is needed."
That's not really heme though. That's everything, including autopsy, though in the latter they tend to add, "In this unfortunate case", which is weird because no death note is going to begin with "Well obviously..." The unfortunate part seems implied.
Heme. Things are difficult. Good difficult, but difficult. I'm starting to absorb the immunostains, which is extremely important in heme. CD20 and CD3 in particular are becoming my bestest friends.
My attending freaks me out a little bit, so I'm just as pleasant (see what I did there) as possible while remaining self deprecating enough to not be aggressively pimped. For instance...
Attending to other resident: Go slowly through this; Ishie won't mind. She's very patient.
Me: It's one of exceedingly few virtues, sir.
Fellow: (chokes)
An interesting thing... I'm either "The Quiet One" (go figure) or "The Extremely Inappropriate One". The former is usually to avoid the latter when I'm around people that I'm not sure will appreciate it, which to be fair, is most people. This occurred in my surgery rotation, which is the only way I made it through the rotation alive. This confused a friend of mine, because the secretary specifically referred to me as the Quiet One, which sparked "Wha??"
The fellow seems to be around me enough to know I'm secretly a horrible person. He hasn't told anyone at this point, so I think we're cool.
Other heme stuff... we work much closer with clinicians, which is cool in a sense, but sucks in a sense, because it means we have to talk directly with people who talk to our patients and they say stuff like "Awww, that's a shame. This kid's so sweet and is such a fighter", and that personal touch is honestly really deflating. Not in a "grave detriment to my work" way by any means, and I do like giving good news on any front, but surgical pathology is quite hands off when people aren't hounding you for frozen sections, and you can be like "Oooh, weird melanoma!", whereas when you see someone's repeat-after-chemo bone marrow packed with Unspeakable Evil and you have to immediately call the clinician, who at times comes down and looks through the scope with you, there's no real excitement to it. "These stain really weird!!!" just doesn't cut it. The heme/onc people are great though. I suppose you'd have to be.
In other news, my mom's coming down to visit for her birthday, so I get to show off Charleston in a hopefully non-murdery, good food sort of way, which contrasts sharply to her last visit which was to a Motel 6 in the hood where someone immediately got killed outside the freeway exit the night we'd gone to a Denny's for dinner. I seem to attract trouble.
Anyhoo: Dear Clinicians, we do actually read your notes. And you are hilarious. "The patient is obese, and extra personnel will be needed in the OR to deal with the obesity of the patient, who I may have mentioned, is obese."
Also, all notes begin "The patient is a pleasant blah blah blah. And all the referrals begin with "Thank you Dr. ScaryName for referring your patient, who is a pleasant blah blah blah". Sometimes, they're "very pleasant". Which of course, is meaningless to us, and after reading thirty notes that begin that way, is either a complete lie, or we have the most pleasant group of in-pain people ever. "The patient, Ms. Jones, is a demanding chore of a woman who has threatened to sue me five times. By referring her to me, I can only guess I have grievously wronged you in some way, and for that, I do apologize."
I know as a medical student, I got some unpleasants. One wanted to be her doctor, which is a story for later and helped me run screaming into my field just in case she ever found me. "My patient, Ms. Really?, said she threatened to slap a nun. I feel no further history is needed."
That's not really heme though. That's everything, including autopsy, though in the latter they tend to add, "In this unfortunate case", which is weird because no death note is going to begin with "Well obviously..." The unfortunate part seems implied.
Heme. Things are difficult. Good difficult, but difficult. I'm starting to absorb the immunostains, which is extremely important in heme. CD20 and CD3 in particular are becoming my bestest friends.
My attending freaks me out a little bit, so I'm just as pleasant (see what I did there) as possible while remaining self deprecating enough to not be aggressively pimped. For instance...
Attending to other resident: Go slowly through this; Ishie won't mind. She's very patient.
Me: It's one of exceedingly few virtues, sir.
Fellow: (chokes)
An interesting thing... I'm either "The Quiet One" (go figure) or "The Extremely Inappropriate One". The former is usually to avoid the latter when I'm around people that I'm not sure will appreciate it, which to be fair, is most people. This occurred in my surgery rotation, which is the only way I made it through the rotation alive. This confused a friend of mine, because the secretary specifically referred to me as the Quiet One, which sparked "Wha??"
The fellow seems to be around me enough to know I'm secretly a horrible person. He hasn't told anyone at this point, so I think we're cool.
Other heme stuff... we work much closer with clinicians, which is cool in a sense, but sucks in a sense, because it means we have to talk directly with people who talk to our patients and they say stuff like "Awww, that's a shame. This kid's so sweet and is such a fighter", and that personal touch is honestly really deflating. Not in a "grave detriment to my work" way by any means, and I do like giving good news on any front, but surgical pathology is quite hands off when people aren't hounding you for frozen sections, and you can be like "Oooh, weird melanoma!", whereas when you see someone's repeat-after-chemo bone marrow packed with Unspeakable Evil and you have to immediately call the clinician, who at times comes down and looks through the scope with you, there's no real excitement to it. "These stain really weird!!!" just doesn't cut it. The heme/onc people are great though. I suppose you'd have to be.
In other news, my mom's coming down to visit for her birthday, so I get to show off Charleston in a hopefully non-murdery, good food sort of way, which contrasts sharply to her last visit which was to a Motel 6 in the hood where someone immediately got killed outside the freeway exit the night we'd gone to a Denny's for dinner. I seem to attract trouble.
Apr 12, 2012
Attempting to be Southern...
Attending: I'm not going to tell you anything about this patient's history; I'm just going to show you the slide. Tell me what you're seeing.
Me: Sickle cell patient
Attending: What cells are you seeing?
Me: Uh... target cells, fragments, reticulocytes, lots of polychromatic forms, SICKLE CELLS
Attending: What cells are these? (points at sickled cells)
Me: Sickle cells
Colleague: Elliptocytes?
Attending: No, not quite elliptocytes. These are sickle cells.
Me: ...
Attending, to me: See right here, this group? (points with scope arrow), they don't look like typical sickle cells, but that's what they are.
Me, flatly: I know.
(pause)
Me: I mean, yes sir.
Surprisingly, the conversation went perfectly normally after that even as my brain was screaming "I SAID SICKLE CELL LIKE FOUR TIMESSSSS IT'S THE ONLY THING I KNOW ASIDE FROM PROSTATE. ACKNOWLEDGE MY GREATNESSSSSS AAAAHHHHH must have theee PREEECCCCIIIOOUUUSSS"
Yeah, I say sir and ma'am now. I pick up strange idiosyncrasies but without the accent or upbringing to back it up. One of my attendings may well be called "Dr. Bless his heart" because he's so damn nice to everyone all the time. "Bless his heart" is a phrase I *NEVER* used before I moved here, and certainly not said in its original intention, but today, while talking to my mom on the phone, I uttered "And Dr. C, bless his heart, actually ordered in bagels from New York for us."
I blame my former roommate for my calling people "doll", "dollface", "baby", and "babycakes" though. People may think I picked them up here, but they were instilled by an exuberant roommate and a lot of burlesque announcers in New York.
The sir thing is weird though. I've never been a sir person, but now it's just part of how I talk to my attendings. "No sir, I'm pulling the patient's history up right now, I apologize for that sir". Every time I do it, in my head, I sound like Bill from True Blood, which eventually means that by the end of my residency, I'm going to have the voice and accent down. Ishie! Did you check the trends on this guy's urine proteins? Sir, I must regret to inform you that those files remain untouched by my hands. Now, if you'll excuse me, sir, I will escort Miss Stackhouse out of the hospital before she surely incites trouble in these halls. Where is that girl... SOOKIE.
Me: Sickle cell patient
Attending: What cells are you seeing?
Me: Uh... target cells, fragments, reticulocytes, lots of polychromatic forms, SICKLE CELLS
Attending: What cells are these? (points at sickled cells)
Me: Sickle cells
Colleague: Elliptocytes?
Attending: No, not quite elliptocytes. These are sickle cells.
Me: ...
Attending, to me: See right here, this group? (points with scope arrow), they don't look like typical sickle cells, but that's what they are.
Me, flatly: I know.
(pause)
Me: I mean, yes sir.
Surprisingly, the conversation went perfectly normally after that even as my brain was screaming "I SAID SICKLE CELL LIKE FOUR TIMESSSSS IT'S THE ONLY THING I KNOW ASIDE FROM PROSTATE. ACKNOWLEDGE MY GREATNESSSSSS AAAAHHHHH must have theee PREEECCCCIIIOOUUUSSS"
Yeah, I say sir and ma'am now. I pick up strange idiosyncrasies but without the accent or upbringing to back it up. One of my attendings may well be called "Dr. Bless his heart" because he's so damn nice to everyone all the time. "Bless his heart" is a phrase I *NEVER* used before I moved here, and certainly not said in its original intention, but today, while talking to my mom on the phone, I uttered "And Dr. C, bless his heart, actually ordered in bagels from New York for us."
I blame my former roommate for my calling people "doll", "dollface", "baby", and "babycakes" though. People may think I picked them up here, but they were instilled by an exuberant roommate and a lot of burlesque announcers in New York.
The sir thing is weird though. I've never been a sir person, but now it's just part of how I talk to my attendings. "No sir, I'm pulling the patient's history up right now, I apologize for that sir". Every time I do it, in my head, I sound like Bill from True Blood, which eventually means that by the end of my residency, I'm going to have the voice and accent down. Ishie! Did you check the trends on this guy's urine proteins? Sir, I must regret to inform you that those files remain untouched by my hands. Now, if you'll excuse me, sir, I will escort Miss Stackhouse out of the hospital before she surely incites trouble in these halls. Where is that girl... SOOKIE.
Apr 8, 2012
Happy Easter!
Dinner will be courtesy of Trader Joe's. I actually googled to see whether there was a TJ's in Charleston when I was moving here, and was bummed that there wasn't, though there's a Whole Foods, and then a month or two after I moved here, they opened one, which makes me way happier than it should since I can't really afford to shop at Whole Foods until I'm an attending.
I'm not sure why I'm expounding on my favorite grocery store. Because I can, I suppose. Anyway, I had aspirations of baking my own ham (for two people) and all sorts of fanciness, then went to the store, saw they had some cheap awesome looking precooked and figured making potato salad and asparagus is enough cooking for a holiday I really only celebrate to score Cadbury eggs.
Speaking of cooking, I literally can't remember the last time I got take out or fast food. That doesn't mean I'm eating healthy or anything (since I learned how to make cupcakes out of alcohol), but it's a huge financial boon, so I took all that newly uneaten money to buy clothes-that-are-not-scrubs because new month new rotation. Since I don't have creepy crawlies, bowel contents, and blood (weirdly) to contend with, I no longer have an excuse to spend all day in my pajamas. Yes hemepath, a field oddly lacking in fresh blood.
See, I took it from grocery stores back to medicine. I'm a jedi. I'm in hematopathology now, which is a field that's in my "maybe I'll do that when I grow up" box without the financial apocalypse that is forensic pathology, which is also interesting, but does not promise to pay off my loans. Also, I hate courtrooms, and considering I just had to rush out to go shopping due to being in another flavor of path, I definitely don't want a closet full of jury fodder to worry about.
ANYway, I initially developed a crush on hemepath when I did pediatric hematology/oncology as my pediatric elective.
For the uninitiated, hematopathology deals with blood (duh) and has a pretty large focus on leukemias, lymphomas, and hemoglobinopathies (like sickle cell), though the former two much more than the latter. Hemepath is much more diagnostic contrasted to blood bank which deals more with obtaining and matching blood, though I actually like both.
Essentially, in hemepath, someone comes in with a blood problem, and we do science at it until we arrive at an answer. We also evaluate treatment, so if someone's been on chemo for a while and their bone marrow is still packed with evil, that's bad. Other stuff. We mostly look at peripheral blood, bone marrow aspirates, bone marrow biopsies, and lymph nodes if they are suspicious for lymphoma. If there are weird blood cells in other body fluids like cerebrospinal fluid or belly juice (usually cytology's turf), we look at that too.
Blood is tricky, because while it may be kind of obvious about being "BAD" or "probably not bad", the different categories of badness look very similar, and knowing whether you have promyelocytic leukemia versus lymphoblastic leukemia versus etc is extremely important for treatment, so we do all sorts of voodoo to these cells and get way more money allocated to play with them. This is in contrast to autopsy where you do not order special stains EVER. "What kind of cancer did they die of? Fatal cancer. Next case."
I'll take a minute to sideline on a couple perception pet peeves here. Cancer is a fantastically expensive set of diseases. It's not anyone's fault. I'd love to blame drug companies and corrupt doctors and government, but cancers are extremely specific self made little assholes, and it takes thousands of hours of manpower and chemical warfare to get into it. A whole spectrum of specialists needs to find out what it is, where it came from, what broke, and then either a magic bullet for it (there are a couple of cancer types that produce a specifically combined gene product that doesn't normally occur and we can target it and kill the cells that make it, but that's unfortunately not many of them) or the specific combination of horrible chemicals that will target the cancer first. A lot of promise in treatment is coming along the way of the understanding of the genome but things like targeted antibodies and the whole new wave thing is outrageously expensive.
I say this to make two points. One. No one can privately afford this. I'm glad that back in someone's grandpa's day, health care was simple and affordable, but if grandpa's sister got leukemia, she'd have died. Two, anyone that says "Sure, we can _____________, but we can't cure cancer!" needs to shut up. Seriously, anything they have to say after that is irrelevant. Most things that can be murdered with a single inexpensive drug (looking at you, syphilis) have been.
I'll also bring up another point, more as an education thing. Since cancer is *not* one disease, approach to treatment is extremely specialized, so anyone thinking "If I got diagnosed with cancer, I wouldn't go through ______", not a good way to look at it. There are pediatric leukemias that have an 80-90% ten year survival rate. The kids lose all their hair, turn white, look like death, get scary pneumonias where they're on a ventilator and you're absolutely certain they're done, and two years later, boom. Hair back, rallied, good grades in school, no cancer. Breast cancer? Runs everything from "not a big deal" to "death sentence". If you ever get cancer, talk extensively with your doctor, look up articles, etc. Also, don't wait because you don't want to deal with it or you don't have the money. Often the only difference between outpatient surgery and stage four metastatic disease is time. Keep in mind, I am *not* saying cling onto the promise of life by your fingernails in the face of everything or that I should manage your individual situation. Believe me, I have a list of cancers and progressive diseases that are in my "Give up and run up all my credit cards in Thailand" category, but I'll be damned if "breast lump" will be one of them.
And please listen to your doctors once you have a diagnosis. If you don't like yours, get a new one, but absolutely consult people with peer reviewed literature on their side *before* and possibly as an adjunct to the other stuff you try. As far as all natural goes, cancer is all natural, which is why you really have to go unnatural to kill it. Lest you think I'm MD patronizing all of you, my grandfather died because of prostate cancer that remained quite treatable until quite late, thus leaving me at 13 with *no* grandparents (last man standing) so it's a topic I care about.
But soapbox off. Where was I? Oh yes, the battery of heme tests. For the most part, heme feels approachable, memorizable. There are nuances to the cells I'm learning to appreciate on morphology, but a lot of it is memorizing which markers correspond to which cells and which markers are likely to go screwy first when the cells they're sitting on go bad.
Unfortunately, one test they run is flow cytometry. Part of tomorrow is going to be spent trying to make heads or tails of it. It's super duper important, and unfortunately, looks like this:
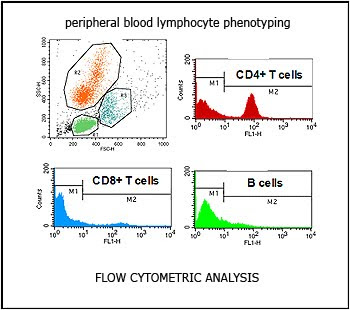
Yeah. When I encountered flow on my first day, a little avatar-Ishie from college calculus popped up, had a seizure, and dropped dead. Lest you think that little graph up there could be comprehended, most flows are about six-ten pages of that run against different parameters and cluster differentiations. So the heme path fellow is flipping through it realllly quickly considering it's full of math and says something to the effect of:
"Okay, it does look like we're dealing with an M4 type acute myelogenous leukemia."
Noooo... it doesn't look anything like acute myelogenous leukemia. AML looks like this:

Whereas that looks like this:

But I'm going to try to get it, so I can pwn hemepath and show it the love I think it deserves.
In the meantime, as your Easter/Game of Thrones Episode 2 present, here's Joffrey getting slapped.

I'm not sure why I'm expounding on my favorite grocery store. Because I can, I suppose. Anyway, I had aspirations of baking my own ham (for two people) and all sorts of fanciness, then went to the store, saw they had some cheap awesome looking precooked and figured making potato salad and asparagus is enough cooking for a holiday I really only celebrate to score Cadbury eggs.
Speaking of cooking, I literally can't remember the last time I got take out or fast food. That doesn't mean I'm eating healthy or anything (since I learned how to make cupcakes out of alcohol), but it's a huge financial boon, so I took all that newly uneaten money to buy clothes-that-are-not-scrubs because new month new rotation. Since I don't have creepy crawlies, bowel contents, and blood (weirdly) to contend with, I no longer have an excuse to spend all day in my pajamas. Yes hemepath, a field oddly lacking in fresh blood.
See, I took it from grocery stores back to medicine. I'm a jedi. I'm in hematopathology now, which is a field that's in my "maybe I'll do that when I grow up" box without the financial apocalypse that is forensic pathology, which is also interesting, but does not promise to pay off my loans. Also, I hate courtrooms, and considering I just had to rush out to go shopping due to being in another flavor of path, I definitely don't want a closet full of jury fodder to worry about.
ANYway, I initially developed a crush on hemepath when I did pediatric hematology/oncology as my pediatric elective.
For the uninitiated, hematopathology deals with blood (duh) and has a pretty large focus on leukemias, lymphomas, and hemoglobinopathies (like sickle cell), though the former two much more than the latter. Hemepath is much more diagnostic contrasted to blood bank which deals more with obtaining and matching blood, though I actually like both.
Essentially, in hemepath, someone comes in with a blood problem, and we do science at it until we arrive at an answer. We also evaluate treatment, so if someone's been on chemo for a while and their bone marrow is still packed with evil, that's bad. Other stuff. We mostly look at peripheral blood, bone marrow aspirates, bone marrow biopsies, and lymph nodes if they are suspicious for lymphoma. If there are weird blood cells in other body fluids like cerebrospinal fluid or belly juice (usually cytology's turf), we look at that too.
Blood is tricky, because while it may be kind of obvious about being "BAD" or "probably not bad", the different categories of badness look very similar, and knowing whether you have promyelocytic leukemia versus lymphoblastic leukemia versus etc is extremely important for treatment, so we do all sorts of voodoo to these cells and get way more money allocated to play with them. This is in contrast to autopsy where you do not order special stains EVER. "What kind of cancer did they die of? Fatal cancer. Next case."
I'll take a minute to sideline on a couple perception pet peeves here. Cancer is a fantastically expensive set of diseases. It's not anyone's fault. I'd love to blame drug companies and corrupt doctors and government, but cancers are extremely specific self made little assholes, and it takes thousands of hours of manpower and chemical warfare to get into it. A whole spectrum of specialists needs to find out what it is, where it came from, what broke, and then either a magic bullet for it (there are a couple of cancer types that produce a specifically combined gene product that doesn't normally occur and we can target it and kill the cells that make it, but that's unfortunately not many of them) or the specific combination of horrible chemicals that will target the cancer first. A lot of promise in treatment is coming along the way of the understanding of the genome but things like targeted antibodies and the whole new wave thing is outrageously expensive.
I say this to make two points. One. No one can privately afford this. I'm glad that back in someone's grandpa's day, health care was simple and affordable, but if grandpa's sister got leukemia, she'd have died. Two, anyone that says "Sure, we can _____________, but we can't cure cancer!" needs to shut up. Seriously, anything they have to say after that is irrelevant. Most things that can be murdered with a single inexpensive drug (looking at you, syphilis) have been.
I'll also bring up another point, more as an education thing. Since cancer is *not* one disease, approach to treatment is extremely specialized, so anyone thinking "If I got diagnosed with cancer, I wouldn't go through ______", not a good way to look at it. There are pediatric leukemias that have an 80-90% ten year survival rate. The kids lose all their hair, turn white, look like death, get scary pneumonias where they're on a ventilator and you're absolutely certain they're done, and two years later, boom. Hair back, rallied, good grades in school, no cancer. Breast cancer? Runs everything from "not a big deal" to "death sentence". If you ever get cancer, talk extensively with your doctor, look up articles, etc. Also, don't wait because you don't want to deal with it or you don't have the money. Often the only difference between outpatient surgery and stage four metastatic disease is time. Keep in mind, I am *not* saying cling onto the promise of life by your fingernails in the face of everything or that I should manage your individual situation. Believe me, I have a list of cancers and progressive diseases that are in my "Give up and run up all my credit cards in Thailand" category, but I'll be damned if "breast lump" will be one of them.
And please listen to your doctors once you have a diagnosis. If you don't like yours, get a new one, but absolutely consult people with peer reviewed literature on their side *before* and possibly as an adjunct to the other stuff you try. As far as all natural goes, cancer is all natural, which is why you really have to go unnatural to kill it. Lest you think I'm MD patronizing all of you, my grandfather died because of prostate cancer that remained quite treatable until quite late, thus leaving me at 13 with *no* grandparents (last man standing) so it's a topic I care about.
But soapbox off. Where was I? Oh yes, the battery of heme tests. For the most part, heme feels approachable, memorizable. There are nuances to the cells I'm learning to appreciate on morphology, but a lot of it is memorizing which markers correspond to which cells and which markers are likely to go screwy first when the cells they're sitting on go bad.
Unfortunately, one test they run is flow cytometry. Part of tomorrow is going to be spent trying to make heads or tails of it. It's super duper important, and unfortunately, looks like this:

Yeah. When I encountered flow on my first day, a little avatar-Ishie from college calculus popped up, had a seizure, and dropped dead. Lest you think that little graph up there could be comprehended, most flows are about six-ten pages of that run against different parameters and cluster differentiations. So the heme path fellow is flipping through it realllly quickly considering it's full of math and says something to the effect of:
"Okay, it does look like we're dealing with an M4 type acute myelogenous leukemia."
Noooo... it doesn't look anything like acute myelogenous leukemia. AML looks like this:

Whereas that looks like this:

But I'm going to try to get it, so I can pwn hemepath and show it the love I think it deserves.
In the meantime, as your Easter/Game of Thrones Episode 2 present, here's Joffrey getting slapped.

Apr 1, 2012
Wahoooooooooooooo
So what, I have a GME presentation and an abstract due because it's SUNDAY SUNDAY SUNDAY...
It's been what... nine months?? I'm all "Dun dun daddda dum, da dum dum daadda dum."
SO freaking excited. Particularly with True Blood and Dexter both being poor showings this last year, I've needed this.
I am being responsible by not going to see Hunger Games with some of the other first years though. Gotta get some work done.
Addendum: Since I haven't geeked out over this show enough, here's some amazing dude playing the opening against multiple copies of himself.
It's been what... nine months?? I'm all "Dun dun daddda dum, da dum dum daadda dum."
SO freaking excited. Particularly with True Blood and Dexter both being poor showings this last year, I've needed this.
I am being responsible by not going to see Hunger Games with some of the other first years though. Gotta get some work done.
Addendum: Since I haven't geeked out over this show enough, here's some amazing dude playing the opening against multiple copies of himself.
Subscribe to:
Comments (Atom)

